Return to CVD Roadmaps Home
The WHF Roadmap on Integrated Care for Cardiovascular Disease (CVD) and Multiple Long-Term Conditions (MLTC) highlights the urgent need to transform health systems that remain largely organised around single diseases. It sets out practical, scalable solutions to support countries in delivering integrated, person-centred care for people living with – or at risk of – CVD and MLTC.
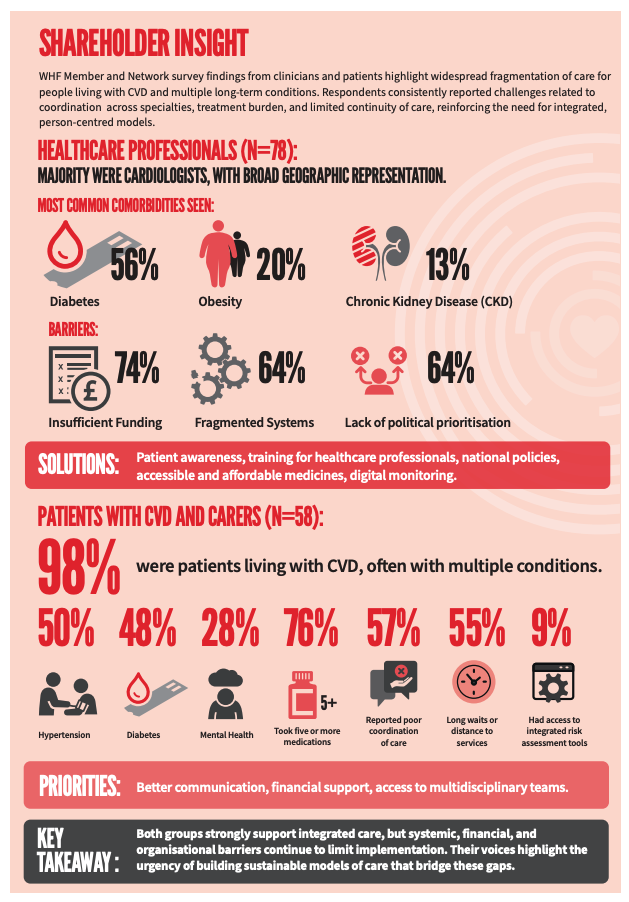
Most people living with CVD also have additional long-term conditions, such as diabetes, chronic kidney disease, and mental health disorders. Yet care pathways remain fragmented, leading to poor coordination, high treatment burden, and suboptimal outcomes.
Why integrated care now
Multimorbidity is the reality.
CVD rarely exists in isolation, requiring coordinated care across multiple conditions and services.
Health systems are not keeping pace.
64% of healthcare professionals identify fragmented systems as a key barrier, alongside insufficient funding (74%) and lack of political prioritisation (64%).
Patients face a high treatment burden.
Complex care pathways, multiple medications, and access barriers make long-term management difficult and unsustainable.
The reality of multimorbidity
Findings from WHF surveys highlight the scale and lived experience of patients:
- 98% of respondents were living with CVD, often alongside other conditions
- 50% reported hypertension, 48% diabetes, and 28% mental health conditions
- 76% take five or more medications
- 57% experience poor coordination of care
- 55% face access barriers, including long waits or travel constraints
- Only 9% report access to integrated risk assessment tools
These findings underline the urgent need to redesign care around patients’ real-life needs.
From fragmentation to integration
The roadmap outlines key priorities to enable integrated, person-centred care:
- Strengthen primary care as the foundation of coordinated services
- Support multidisciplinary teams to manage complex patient needs
- Improve coordination across services and providers
- Leverage data systems and digital tools for continuity of care
- Expand access to essential diagnostics and technologies
Healthcare professionals also highlight actionable priorities, including improving patient awareness, strengthening workforce training, implementing national policies, expanding access to affordable medicines, and using digital monitoring tools.
The evidence at a glance
Integrated care can:
- Improve clinical outcomes for people with CVD and MLTC
- Reduce treatment burden and improve quality of life
- Increase efficiency and sustainability of health systems
- Promote equitable access to care across populations
Benefits of integrated care
Integrated, person-centred approaches help:
- Deliver care that reflects patients’ real-life needs and contexts
- Reduce duplication and fragmentation across services
- Strengthen continuity of care over time
- Improve patient experience and engagement
Common barriers — and how to solve them
Fragmentation of services
Strengthen primary care and coordination mechanisms
Limited funding and resources
Prioritise integrated care in national health strategies and budgets
Lack of policy prioritisation
Align governance frameworks and national NCD plans
Workforce and training gaps
Invest in multidisciplinary training and capacity building
Limited use of digital tools and data systems
Scale up digital health solutions and integrated data platforms
A call to action
Integrated care for people living with – or at risk of – CVD and MLTC must be implemented urgently.
This requires:
- Aligned policies and governance
- Shared leadership across sectors
- Patient and community engagement
- Targeted investment, particularly in primary care
As multimorbidity continues to rise, the opportunity is clear: translate evidence into action and build health systems that are equitable, resilient, and centred on people—not diseases.

Global CVD Roadmaps











